Email: info@BSBortho.com
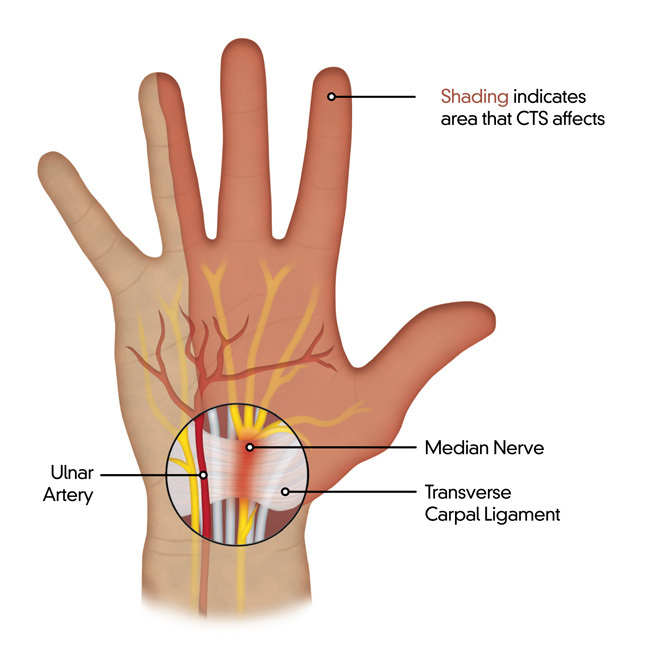
Carpal tunnel syndrome (CTS) occurs when the median nerve is compressed as it travels through the carpal tunnel in the wrist, causing pain, numbness, weakness and tingling in the hand.
Patients will often report:
Carpal tunnel syndrome is typically a clinical diagnosis, based on a detailed history and physical exam. The following tests can be ordered as part of your workup to confirm the diagnosis.
Radiographs/X-rays
These may be ordered to rule out other causes of wrist pain.

Electromyography (EMG) / Nerve conduction study (NCS)
Ultrasound (US)

In severe cases, where symptoms do not respond to non-surgical treatment, surgery has been shown to be an effective method for treating carpal tunnel syndrome. Various techniques have been shown to be effective, with no single technique deemed superior based on the current evidence [Pace et al, 2023]. However these techniques have specific advantages and disadvantages, and should be taken into account when choosing among the surgical methods.
Open Carpal Tunnel Release
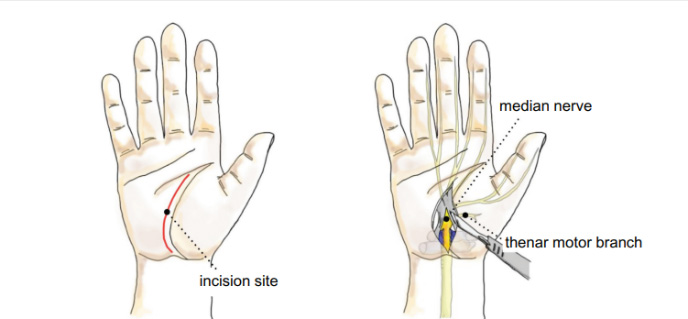
An open carpal tunnel release uses a traditional incision or mini-incision along the distal wrist crease. The most common length of the traditional incision is 5 cm and mini-incision is 2 cm. [Pace et al, 2023]. The incision is extended through the palmar fat and fascia, and then the transverse carpal ligament is completely split longitudinally. The wound is closed with stitches.
Open carpal tunnel release has been reported to be safe overall, but complications include wound infection, nerve injury and scar formation, especially using a traditional size incision.
Endoscopic carpal tunnel release
The endoscopic carpal tunnel release uses a single or two-portal approach, and was first introduced in 1986 [Okutsu et al, 1986]. The endoscopic technique uses a small camera to look into the carpal tunnel and cut through the transverse carpal ligament.
The endoscopic carpal tunnel release has good reported outcomes with a low complication rate and better esthetic results due to the smaller scar.
Ultrasound-Guided carpal tunnel release (US-CTR) uses ultrasound to visualize the median nerve and transverse carpal ligament, and perform the release. The ultrasound-guided approach has been shown to have a low complication rate and fast recovery. [Sanati et al, 2011; Chou et al, 2022; David, 2022; Moungondo and Feipel, 2022].

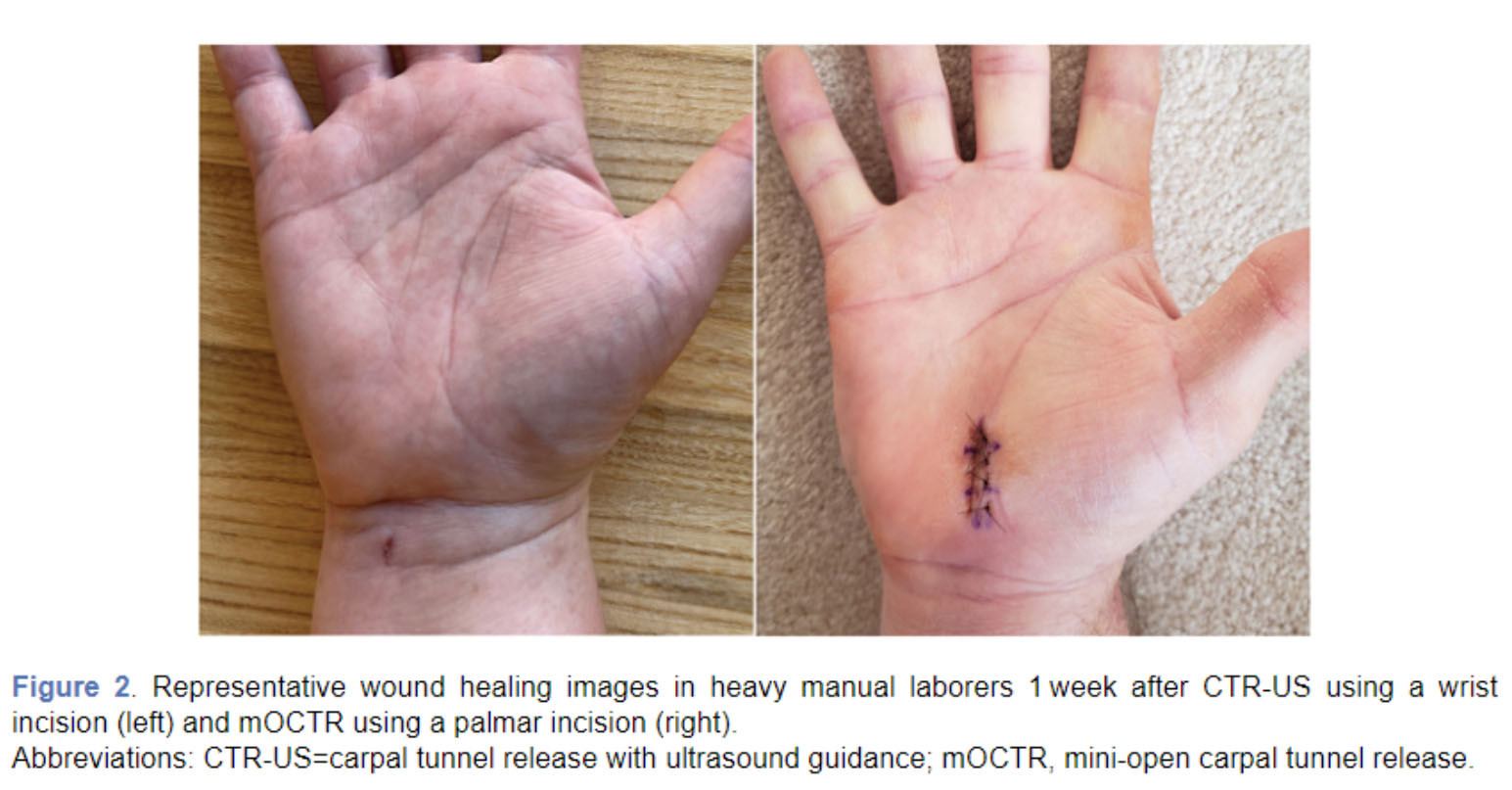
The Sonex SX-One MicroKnife is a new, cutting-edge device designed to further improve the success and the safety of ultrasound guided carpal tunnel releases. The technique is performed using only local anesthetic and is inserted through a 2-4 mm incision (compared to 20-50 mm in open surgery). The device deploys miniature balloons to protect important structures and increase the space for the knife to transect the transverse carpal ligament. These balloons, and the proprietary cutting device, prevent unintended injury to nearby neurovascular structures and adjacent soft tissue which could prolong recovery.
In a recent ground breaking study, titled “Multicenter Randomized Trial of Carpal Tunnel Release with Ultrasound Guidance versus Mini-Open Technique,” orthopedic hand surgeon Dr. Kyle Eberlin (Program Director, Harvard Plastic Surgery Residency Program, and Associate Program Director, MGH Hand Surgery Fellowship) found that USG-CTR performed equally to the mini-open surgical carpal tunnel release. The authors found no statistical differences between the groups, except they did find that USG-CTR group reported “freedom from pain and wound sensitivity” in 61% of patients, compared to in only 18% of mini-open CTR patients.[Eberlin 2023]
Boston Sports & Biologics is now the 2nd location on the East Coast to perform the Thread Carpal Tunnel Release (The Guo Technique).
This minimally invasive treatment uses just a needle and a thread to release the transverse carpal ligament; there is no blade or scalpel involved. It is performed in the office, under ultrasound guidance using only local anesthesia, in an average of 15 minutes. Patients are generally able to return to their normal activities of daily living that day and depending on their job return to work the next day or next week.
References: